Groin hernia (Inguinal Hernia and Femoral Hernia) in Adults
What is a groin hernia?
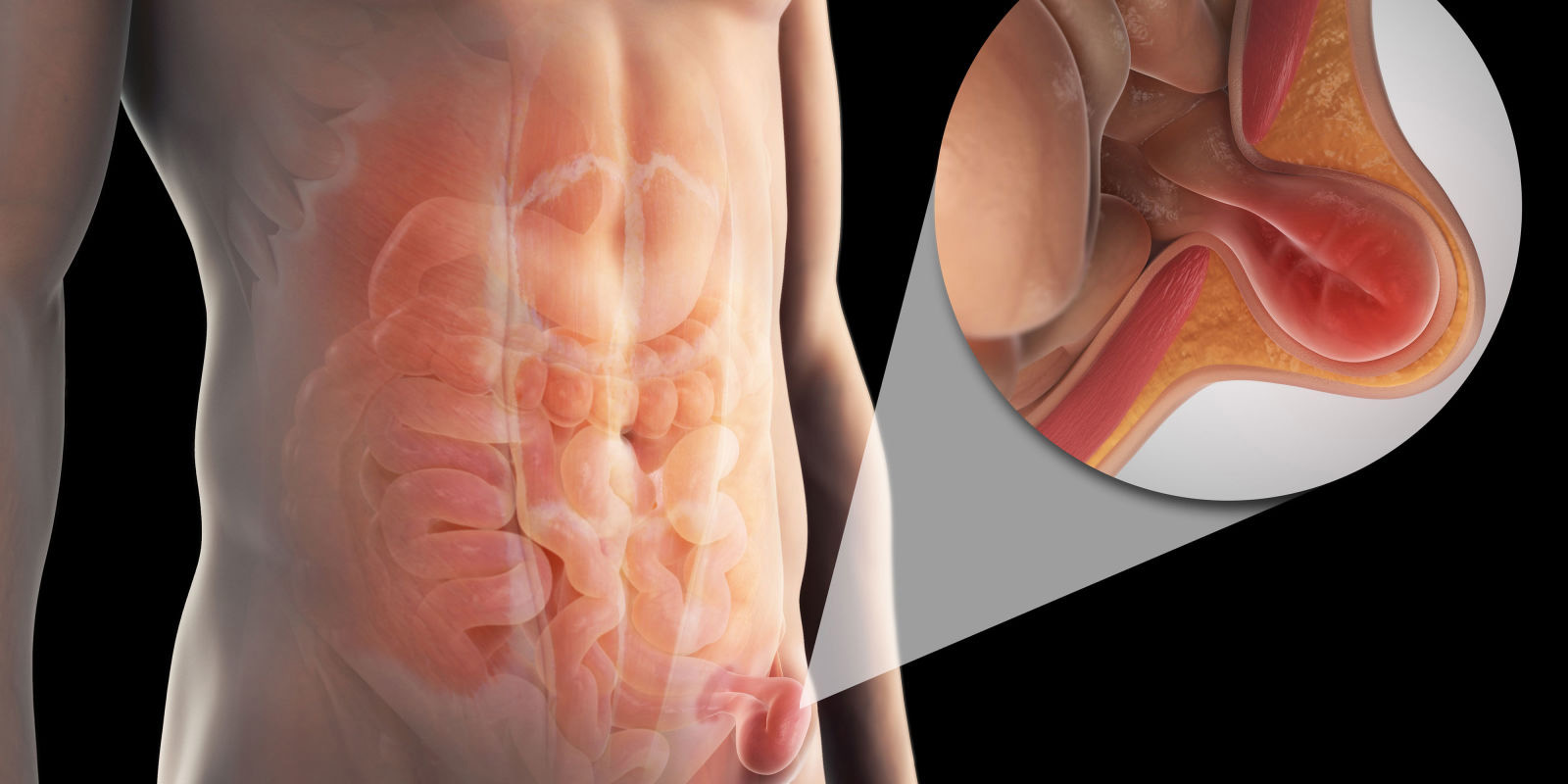
“Groin hernia” are common. The most common type is an inguinal hernia, which accounts for over 75% of all groin hernia. Rarer is a femoral hernia.
A hernia occurs when there is a weakness of the abdominal wall, and contents of the abdominal cavity push through this weakness. In the case of groin hernia, the weakness is through the inguinal canal (https://en.wikipedia.org/wiki/Inguinal_canal) or femoral canal (https://en.wikipedia.org/wiki/Femoral_canal). This leads to in a bulge in the groin, which is often worse on standing, and when coughing or straining. It may disappear (or reduce) when lying down or with gentle manual pressure.
Symptoms of a groin hernia
Groin hernia may cause a variety of symptoms. Some people will notice either a bulge or pain in the groin, often exacerbated by lifting and straining. The pain can range from a dull aching sensation though to sharp severe pain. On occasion a groin hernia does not cause any symptoms; this is termed an asymptomatic hernia. Typically symptoms are worse towards the end of the day, particularly after long periods of standing or activity. The pain and discomfort can limit a person’s activity and this may result in time off work. Over time groin hernia tend to increase in size and become more uncomfortable.
Complications of a groin hernia
Complications can occur with groin hernia. An incarcerated hernia means the hernia is no longer reducible, in other words the hernia is unable to be pushed back inside. When this occurs more serious complications become more likely.
Strangulation is a term for when the contents of the hernia become tightly “trapped” within the hernia and they lose their blood supply. A strangulated hernia is a potentially a serious and life threatening complication. At times the intestine can become trapped within the hernia, which can lead to bowel obstruction, another potentially life threatening complication. If you have very painful hernia, which is either “stuck” or is red or tender seek medical attention as soon as possible.
Femoral hernias are much more likely than inguinal hernia to lead to bowel obstruction or strangulation.
Risk Factors for Groin Hernia
Approximately 25% of men and 5% of women will develop in groin hernia in their lifetime. Inguinal hernias are the most common hernia. They occur much more frequently in men than in women. Femoral hernias are more common in women, although an inguinal hernia is still the most common groin hernia in a woman.
Groin hernia occur as a result of weakness of the abdominal wall, this can either be a congenital (birth defect) or an acquired weakness related to aging and weakening of the abdominal wall tissues and muscles. Other factors that contribute to development of a hernia include anything that increases abdominal pressure, such as chronic coughing, constipation, strenuous exercise and heavy lifting.
Treatment of Groin Hernia
Inguinal hernias do not heal by themselves. The only way to get rid of a hernia is by surgery. There are several different operations available for repair of an inguinal hernia.
An “open” approach involves an incision to the lower part of the abdomen. The cut is normally about 7-10cm long. The inguinal canal is opened, the peritoneal sac is either excised or reduced and usually a mesh (often polypropylene) is inserted and secured in place covering the affected area.
A “laparoscopic” or keyhole approach involves entering the abdomen, usually near the umbilicus (belly button) and placing 2 further small cuts to on either side of the abdomen. Using keyhole instruments, the hernia sac is reduced from inside the abdomen, and a mesh is placed between the peritoneum and abdominal wall. Sometimes this is held in place with sutures or laparoscopic tacks.
Hernia repair is usually carried as a day case procedure. An open repair can be carried out under local or general anaesthetic. However laparoscopic repair can only be performed under general anaesthesia.
Your surgeon will discuss with you the risks and benefits of the different surgical options. Information is available from NICE: (https://www.nice.org.uk/guidance/ta83/chapter/1-Guidance)
Should a hernia always be repaired?
If an inguinal hernia is very small or is asymptomatic it may be left alone. However hernia tend to enlarge over time and both UK and US trials have demonstrated that most men with an asymptomatic hernia will require surgery as a result of increasing pain. In general the smaller the hernia the easier it is to “fix”. Surgical repair reduces the potential risk of serious hernia related complications later on.
Symptomatic inguinal hernia would usually be offered repair with the aim of alleviating symptoms and improving quality of life.
Because of the high risk of strangulation, femoral hernia would usually be repaired relatively urgently regardless of whether it’s symptomatic or not.
Sometimes wearing a truss may help to relieve the discomfort of a hernia. This will not get rid of the hernia however.
Risks and Complications of surgery
Generally speaking groin hernia surgery is very safe with a low risk of complications.
Following surgery most patients will experience some discomfort and some minor swelling at the operation site. Patients will be given painkiller medication for this, and this is usually only necessary for the first few days after surgery. There may also be some bruising, and in men the scrotum may be swollen for a few days. There is a small risk that patients may not be able to pass urine following surgery, if this occurs a catheter is usually required.
Complications of the operation include:
Infection
A wound infection involves the scars, which then become hot, red, swollen and painful. There is sometimes discharge from the wound. Some wound infections require a short course of antibiotics, more rarely a further operation is required.
Mesh infection is rare. However when a mesh becomes infected it is more difficult to treat. Often this requires a prolonged course of antibiotics, sometimes intravenously. If the infection does not resolve the mesh may need to be removed with an operation. Mesh infection is less common with laparoscopic repair (0.1%) compared to open repair (0.5%).
Bleeding
Minor bruising is common following hernia surgery. Significant bleeding is very rare. Any bleeding is controlled at the time of the operation, but afterwards there is small chance bleeding can occur. This can lead to a haematoma either related to the wound, inside the abdomen, or into the scrotum. Should this occur it tends to resolve gradually over a few weeks. It is possible, albeit extremely unlikely that a blood transfusion is required. Sometimes further surgery is required. With laparoscopic groin hernia surgery there is a very small risk of damage to the large groin vessels (iliac and femoral vein). This is a serious complication and will be dealt with during the operation, often needing open surgery. Fortunately this is exceptionally rare.
Visceral injury
Whenever bowel is handled there is small possibility of damaging the bowel. In open groin hernia surgery this can occur rarely but is more common with laparoscopic surgery. It is still however rare. Recognised injuries will be repaired during the operation. If this is not recognised further surgery may be required. Other than bowel the bladder can sometimes be damaged. Again this is exceptionally rare.
Chronic pain and nerve injury
A minority of patients have on-going pain in the groin following surgery. This is caused by nerves that run in the groin which get handled during the operation, or get pressure from scar tissue that forms post operatively. The risk of chronic groin pain is lower with laparoscopic surgery. After open surgery there is often a numb patch at the base of the penis, which slowly resolves over time, but is occasionally permanent.
Hernia recurrence
There is no method of hernia repair that can give a 100% guarantee that it won’t recur. Inguinal hernias recur in about 0.5 – 3 % of cases treated. If it does recur a repeat operation is often required.
Testicular ischaemia
In men inguinal hernia develop very close to the structures that run to and from the testicle. Hernia repair is associated with a small risk of damage to these structures which can lead to painful swelling of the testicle, and later shrinkage of that testicle. Very rarely this can lead to reduced fertility or necessitates the testicle to be removed.
General risks of surgery and anaesthesia
Modern anaesthetics are very safe. Most people are not affected. Rarely some patients develop a reaction to the anaesthetic, or develop a blood clot in the leg (deep vein thrombosis) that can go to the lung (pulmonary embolism). Patients at risk of this are given compression stockings (TEDS) to wear. Very rarely patients may suffer a heart attack or a stroke as result of anaesthesia and surgery.
After your operation
Following discharge from hospital the area around the hernia operation may be sore for the first few days. You will be given painkiller medication, take these as prescribed. The wound would usually be closed with dissolvable stiches which do not need to be removed. You can shower and bath after 24 hours. Spare dressings and instructions will be provided on discharge.
There are no restrictions on diet following surgery. However it’s advised, for the first 3-5 days to eat relatively light and bland food, and avoid fizzy drinks.
After surgery it is best to walk and mobilise gently, and gradually build up to normal activity as you feel able and pain allows. You should avoid heavy lifting for the first 4 to 6 weeks following surgery. Providing you have no discomfort it is ok to do cycling, swimming and running within about 2 weeks of surgery.
You should be able to drive after about 7-10 days. You must be able to look over your shoulder as normal, and perform an emergency stop without pain or discomfort. If in doubt practice this first before driving.
Going back to work depends on your job. Most patients who have sedentary jobs are able to return to work by about 2 weeks. If your job involves heavy lifting or manual labour then 4-6 weeks off work is required.
Complications after discharge are unusual. After private surgery we will phone you on a daily basis for the first few days. You will be given emergency contact details, which you should call if you think something may be wrong.